
Frailty and Polypharmacy Risk Calculator
This tool helps assess your risk of medication-related side effects based on the number of medications you take and your frailty status. For best results, discuss your scores with a healthcare professional.
Your Risk Assessment
What You Should Know
When an older adult takes five or more medications daily, it’s not just a numbers game-it’s a ticking time bomb. For many seniors, especially those who are frail, each pill adds up, not in healing, but in risk. Dizziness. Falls. Confusion. Constipation. These aren’t just side effects; they’re warning signs that the medicine list has outgrown its purpose. And the worst part? It’s happening to millions. In the U.S., nearly half of all older adults are on five or more medications. For those in nursing homes, it’s over 96%. But here’s the truth: polypharmacy isn’t always the answer-it’s often part of the problem.
What Exactly Is Frailty, and Why Does It Matter?
Frailty isn’t just being old or slow. It’s a medical condition defined by five clear signs: unintentional weight loss, feeling exhausted most days, weak grip strength, walking slower than usual, and low physical activity. If you have three or more of these, you’re frail. If you have one or two, you’re pre-frail-and that’s still a red flag. Frailty doesn’t just make you tired. It makes your body less able to handle stress, including the stress of medications.
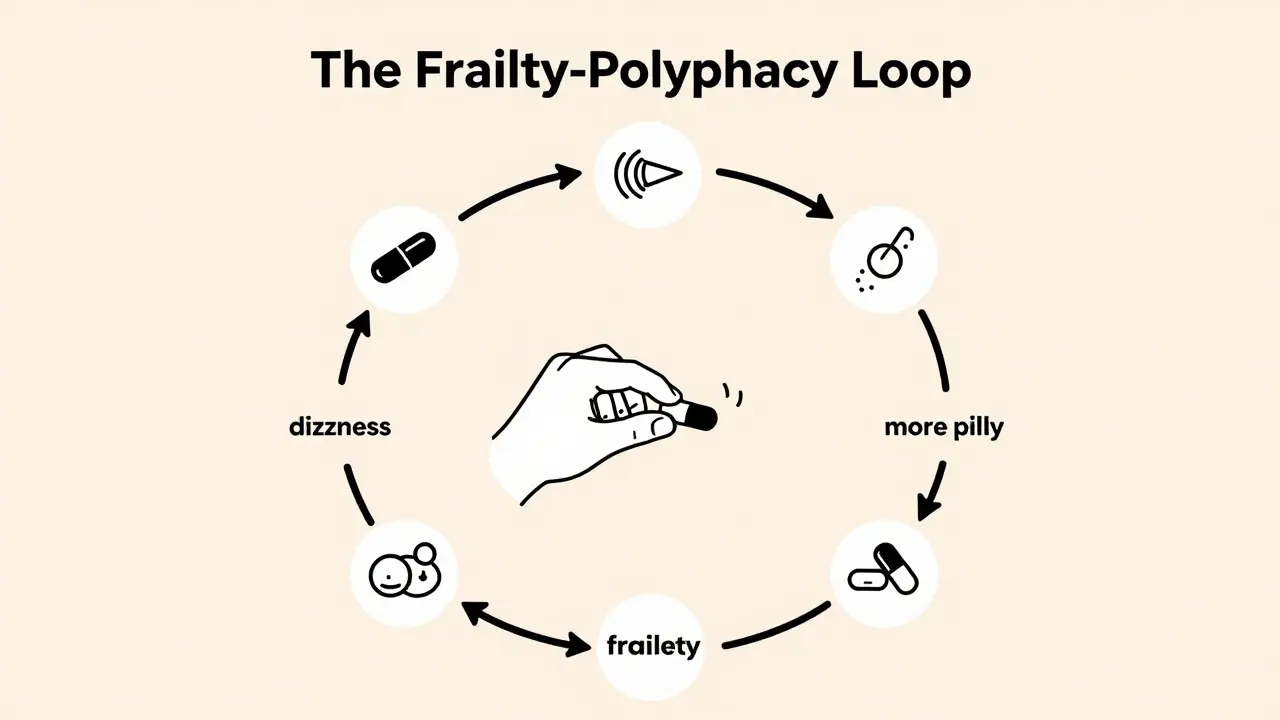
Studies show that 75% of older adults on five or more drugs are either pre-frail or frail. And it’s not just correlation-it’s a cycle. Each extra pill increases the chance of frailty by 12%. At the same time, frail people are more likely to be prescribed more drugs because they have more health problems. So you get stuck: more drugs → more frailty → more drugs.
Polypharmacy: More Pills, More Problems
Polypharmacy means five or more medications taken daily. But here’s what most people don’t realize: it’s not the number that’s the issue-it’s the *inappropriateness*. Many of these drugs were prescribed years ago, for conditions that have since changed. Or they’re duplicates. Or they interact dangerously. A 73-year-old with heart disease might be on blood pressure meds, diabetes drugs, cholesterol pills, a blood thinner, and a sleep aid. That’s five right there. Add in an antacid, a painkiller, and a vitamin, and you’re at eight. No one stopped to ask: "Do we still need all of these?"
What’s worse? The side effects pile up. In nursing homes, 73% of residents on eight or more medications report constipation. Over 60% say they feel dizzy. Nearly half have fallen in the past year. And 42% admit they skip doses because the routine is too confusing. That’s not compliance-it’s survival.
And the costs? They’re staggering. In the U.S., medication-related problems cost $30 billion a year and contribute to 30% of hospital admissions in seniors. Around 125,000 to 300,000 preventable deaths each year are tied to improper drug use in older adults. These aren’t statistics-they’re people. Grandparents. Neighbors. Your own family.
The Bidirectional Trap: How Frailty and Polypharmacy Feed Each Other
This isn’t a one-way street. Frailty makes someone more sensitive to drugs. Their kidneys and liver don’t clear medications as well. Their body weight changes. Their brain reacts differently. So a dose that was fine at 65 becomes dangerous at 75. Meanwhile, those same drugs-especially sedatives, anticholinergics, and blood pressure pills-can cause dizziness, confusion, and muscle weakness. That leads to falls. Falls lead to hospitalization. Hospitalization leads to more drugs. More drugs lead to more frailty.
One study found that taking seven or more medications over eight years doubled the risk of becoming frail. Another showed that for every additional pill, the odds of frailty rose by 12%. And when researchers looked at quality of life, they found something shocking: frailty and polypharmacy didn’t just coexist-they *mediated* each other. Meaning, one made the other worse. It’s a loop with no easy exit.
Who’s Most at Risk?
It’s not random. Women are more likely to be on multiple drugs than men. Non-Hispanic White seniors have higher rates than Black or Hispanic seniors. Those with less education are more likely to be overwhelmed by their pill boxes. And people with heart disease? They’re the most affected. Over 60% of them are on five or more medications. Diabetes? Over 50%. Hypertension? Nearly 50%.
And where you live matters. In your home? About 4% of seniors are on five or more drugs. In the hospital? Over 96%. That jump isn’t because they got sicker-it’s because every specialist adds their own list. A cardiologist adds one. A neurologist adds another. A rheumatologist adds three. No one looks at the whole picture.
What Can Be Done? The Path to Deprescribing
The good news? You can take back control. It’s called deprescribing-not stopping everything, but carefully removing drugs that don’t belong anymore. And it works.
The Beers Criteria and START/STOPP guidelines are the gold standards. They list drugs that should be avoided in older adults and ones that are often missed. When clinics use them, inappropriate prescribing drops by 30-50%. But they’re only useful if someone actually uses them.
One successful method is the "3-Step Method" from Johns Hopkins:
- Review-Look at every pill, patch, and spray. Ask: "Why was this prescribed? Is it still needed?"
- Discuss-Talk to the patient. "What are you worried about if we stop this?" "What are your goals?" Many seniors just want to feel better, not take more pills.
- Monitor-Check in after 2 weeks. Watch for changes in energy, balance, appetite, or mood.
Studies show this approach reduces inappropriate medications by 28% in six months-with 92% of patients sticking to the plan. And here’s the kicker: 76% of people in the EMPOWER trial felt better after stopping one or more drugs. No crashes. No rebound. Just more energy, fewer falls, and better sleep.
Who Should Lead This Change?
It’s not just the doctor’s job. Pharmacists are the unsung heroes here. In places where pharmacists lead medication reviews, adverse events drop by 34%. Geriatric clinics that do full assessments reduce polypharmacy by 22% in a year. And patient education helps too. The "Medication Check-Up" program improved understanding by 47%-meaning seniors could finally explain what they were taking and why.
Technology is catching up too. In January 2024, the FDA approved the first AI-powered tool called MedWise Risk Score. It analyzes all your meds and flags dangerous interactions. In trials, it cut adverse events by 37%. And tools like Medisafe and Round Health help seniors track pills, set reminders, and even share their lists with caregivers.
Why Do Doctors Keep Prescribing?
It’s not laziness. It’s time. Most primary care doctors spend 15-20 minutes per visit. Reviewing a full medication list takes longer. And many don’t know how. Only 38% of U.S. hospitals have electronic alerts for inappropriate drugs. And 61% of doctors say they rarely consider deprescribing because they’re too busy.
Plus, patients are scared. Half of seniors worry that stopping a drug will make them sicker. They’ve been told for years: "Take it every day. Don’t miss a dose." So even when the doctor suggests stopping, the patient says no.
What’s Changing Now?
The tide is turning. In 2023, the American Geriatrics Society launched the "Age-Friendly Health Systems" initiative. Over 2,850 hospitals now follow the 4Ms: What Matters (the patient’s goals), Medication (right drugs, right dose), Mentation (brain health), and Mobility (movement). The result? A 24% drop in inappropriate polypharmacy.
The NIH is funding a $15 million trial called FRAIL-PHARM, testing a pharmacist-led intervention for frail seniors. The WHO is pushing for a global goal: cut severe medication harm by 50% by 2030. And the market for deprescribing software? It’s growing from $185 million to $412 million by 2028.
But real change happens one person at a time. One review. One conversation. One pill taken off the list.
What You Can Do Today
If you’re caring for an older adult-or if you’re one-here’s how to start:
- Get a full list of every medication, supplement, and OTC pill. Include creams, patches, and inhalers.
- Ask the doctor: "Which of these are still necessary? Which might be doing more harm than good?"
- Bring up frailty. Say: "I’ve noticed [name] is more tired, slower, or has fallen once. Could this be linked to the meds?"
- Request a pharmacist-led medication review. Many insurance plans cover this now.
- Use a pill tracker app. It helps spot duplicates and missed doses.
- Don’t be afraid to ask: "What happens if we stop this?"
Medicines aren’t the enemy. But too many, at the wrong time, can become a burden. The goal isn’t to take fewer pills-it’s to take the right ones. And for someone who’s frail, sometimes the best medicine is the one you don’t take anymore.
matthew runcie
March 22, 2026 AT 08:28Just sayin'.
shannon kozee
March 23, 2026 AT 15:31Shaun Wakashige
March 24, 2026 AT 13:04Solomon Kindie
March 26, 2026 AT 08:09Johny Prayogi
March 26, 2026 AT 09:03Desiree LaPointe
March 26, 2026 AT 20:05Jackie Tucker
March 28, 2026 AT 14:47trudale hampton
March 29, 2026 AT 17:38Timothy Olcott
March 30, 2026 AT 13:01Paul Cuccurullo
March 30, 2026 AT 20:55Allison Priole
April 1, 2026 AT 10:43